Subscribe to get full access to this operation and the extensive Shoulder & Elbow Surgery Atlas.
FREE TRIAL
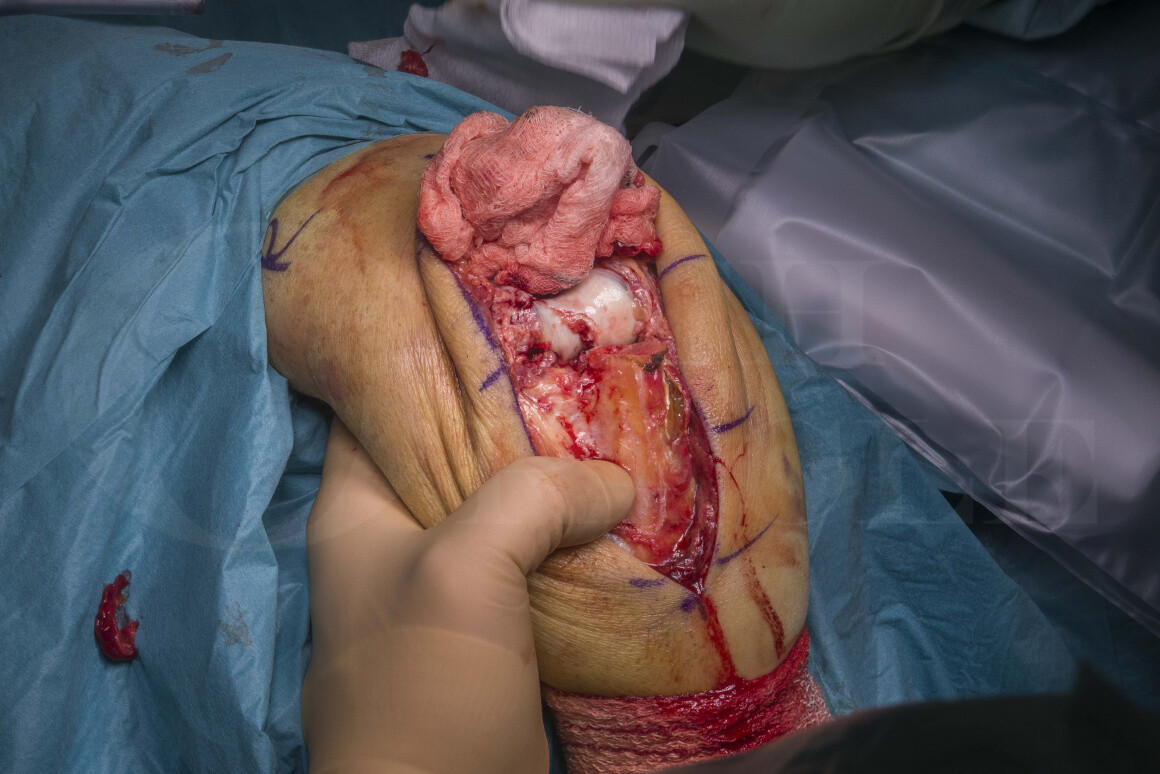
Learn the Distal humeral coronal shear fracture: Open reduction and internal fixation using Medartis CCS headless screws using trans-olecranon approach(Synthes LCP hook plate) surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Distal humeral coronal shear fracture: Open reduction and internal fixation using Medartis CCS headless screws using trans-olecranon approach(Synthes LCP hook plate) surgical procedure.
Distal humerus fractures cover a range of complex fracture patterns including supracondylar fractures, single or bi-column fractures and coronal shear fractures. They account for approximately 7% of all fractures. They have a bimodal distribution with the first peak in 20 and 30 year old males, and a second peak in the over 70s and is more common in females. The most common type are the distal intercondylar fractures, with coronal shear fractures being much less common (6%0 of distal humeral fractures). In our unit, we tend to see 2-5 cases per year.
Comminuted fractures of the distal humerus and, coronal shear fractures in particular pose a technical challenge for the upper limb orthopaedic surgeon. Although there have been advances in implants coming to market, these fractures are commonly technically difficult to access and technically difficult to secure a robust fixation due to the limited access and bone stock available for fixation. It is associated with high complication rates and poor clinical outcomes. Comorbidities, including diabetes, osteoporosis and combinations of severe soft tissue damage, worsen the healing capacity.
The method of surgical management of this subset of fractures is largely determined by the age and function of the patient, and the complexity of the fracture.
In broad principles, younger patients will undergo open reduction and surgical fixation to try to preserve the native bone. In pure coronal shear fractures, the lead author tends to fix using headless screws. Depending on fracture complexity and characteristics, this may be augmented with dorsal locking plates if there is concern regarding biomechanical stability of the fracture.
In older patients with lower functional demand, where the bone can be osteopaenic and more comminuted, fixation may be less reliable. In these cases, elbow arthroplasty in the form of elbow hemiarthroplasty or total elbow replacement may be the more reliable option. Concerns regarding longevity in elbow arthroplasty patients remain, and therefore, tend to be an option of last reserve.
The greatest difficulty is selecting the correct operation in active patients in the 50-60s age group is that they tend to have challenging fracture patterns with varying levels of osteopaenia. Ultimately, the aim is a pain-free, functional elbow. If a stable fixation can be achieved, this would be preferred to arthroplasty.
If surgical fixation is planned, the lead author tends to commit to performing an olecranon osteotomy to maximise the operative exposure and to ensure the best chance of fixation.
If a stable fixation is not achievable, an elbow hemiarthroplasty is still a viable bailout option with an olecranon that has been osteotomised. Smith et al. reported a series of 23 patients showing good outcomes after elbow hemiarthroplasty and olecranon osteotomy.
For coronal shear fractures, as the fracture fragments are largely intra-articular, a headless screw option is ideal for these fracture patterns. A cannulated system gives advantage for complex fracture fixation, where K-wires can be used to temporarily stabilise fracture fragments which in turn ensure appropriate screws positioning without the use of additional K-wires.
I prefer using the Medartis Cannulated Compression Screw (CCS) system due to the flexibility of options it offers. This system has a wide range of titanium screw diameters from 1.7mm up to 7.0mm and lengths (ranging from 10 – 40mm). They come in headed and headless options as well has having short and long thread options. They also have percutaneous instrumentation if the opportunity arises.
The main advantage over other headless screw systems is that once a wire has been sited, a headless screw can be applied directly without reaming the bone due to the presence of a cutting thread on the screw. This feature is most useful for complex and unstable fracture patterns. Reaming can often lead to loss of position as the hold in the bone is lost during this step.
For coronal shear fracture, the most common diameters are the 2.2 or 3.0mm diameter screws.
OrthOracle readers will find the following associated operative techniques also of interest:
Distal Humeral fracture(Hoffa type): Internal fixation with Medartis plate
Humeral fracture: Transcondylar distal fracture fixation with Synthes 2.7mm/3.5mm Variable Angle Locking Compression Plate, triceps sparing approach
Humeral fracture: Fixation of distal third fracture using Synthes LCP extra-articular distal humeral plate
Total elbow replacement using the Coonrad-Morrey Total Elbow Replacement (Zimmer-Biomet)
Author: Sam Chan FRCS (Tr & Orth)
Institution: The Queen Elisabeth Hospital, Birmingham, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













