Subscribe to get full access to this operation and the extensive Bone & Soft Tissue Tumour Surgery Atlas.
FREE TRIAL
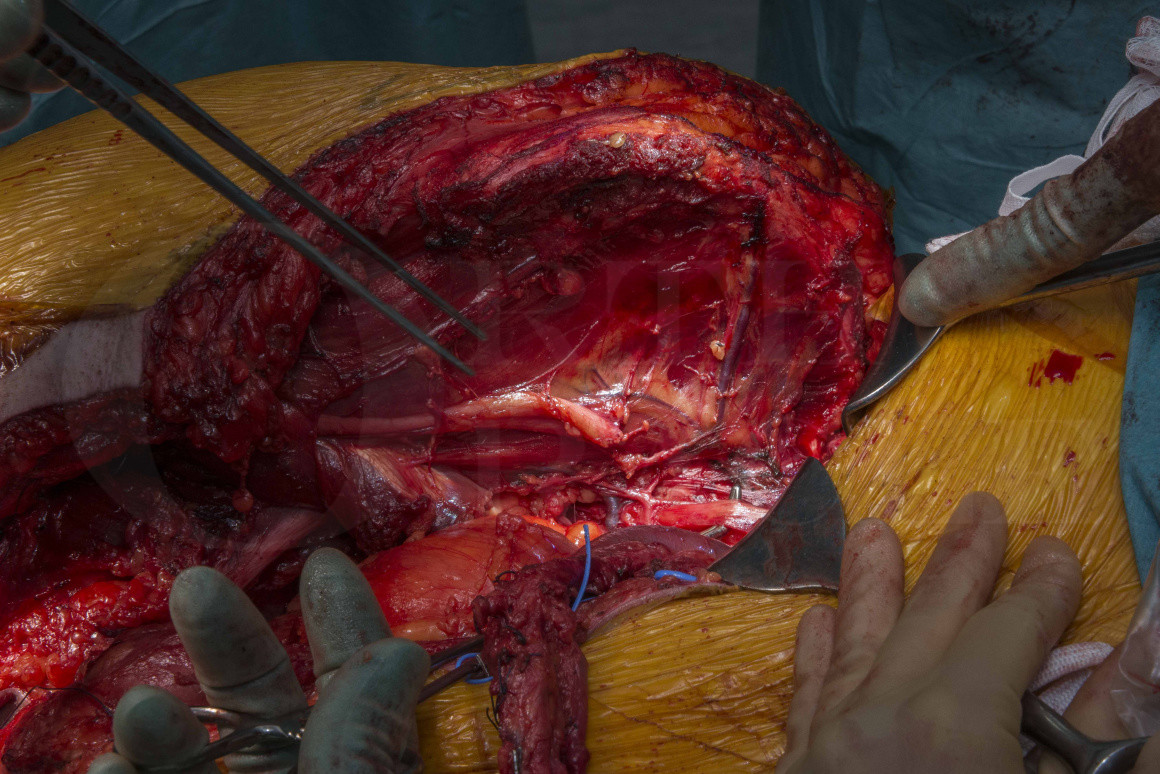
Learn the Hindquarter amputation: with pedicled fillet flap for chondrosarcoma of the proximal femur surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Hindquarter amputation: with pedicled fillet flap for chondrosarcoma of the proximal femur surgical procedure.
Pelvic resections remain the most challenging of procedures for patients and surgeons alike. Regrettably there are occasions when a tumour cannot be excised without sacrificing the limb, necessitating a hindquarter amputation.
When tumours arise in the limbs, oncology surgeons need to consider the contamination of each individual compartment when planning the surgical strategy. Where a tumour has undergone inadvertent surgery, contamination of many compartments can occur and significantly impact upon the potential to salvage a limb. At the hip, if multiple compartments and the hip joint are contaminated by tumour, then only a hindquarter amputation or rotationplasty (where a femoral tumour is excised and the ankle rotated to become and functional ‘knee’ joint) offer a curative option for a chemo-radiotherapy insensitive tumour such as clear cell chondrosarcoma. In principle, limb-salvage may still be possible in chemo-radiosensitive tumours such as Ewing’s sarcoma or in some oligometastatic bone tumours.
The British Orthopaedic Oncology Society have produced helpful guidelines to minimise the chance of inadvertently operating on tumour cases, with the attendant risks including compromising the possibility of limb salvage surgery. The key point is that prodromal pain and injury mechanisms not in keeping with traumatic fractures are indicative of pathological fractures i.e. due to an underlying cause such as malignancy (or osteoporosis, infection, metabolic disease, dysplasia, Paget’s disease etc). In such cases there is no rush to stabilise fractures (STOP), patients should be investigated throughly including whole-body staging (SCAN) and discussed with their treating oncologist if metastatic or with a specialist orthopaedic oncologist if solitary (PLAN).
OrthOracle readers will also find the following operative techniques of interest:
Computer navigated P1 hemipelvectomy for chondrosarcoma and GRAFTJACKET (Wright Medical) reconstruction
Computer navigated Hemi-pelvectomy for Ewings sarcoma
Hindquarter amputation (for pelvic soft tissue sarcoma)
Author: Jonathan Stevenson FRCS (Tr & Orth)
Institution: Royal Orthopaedic Hospital, Birmingham, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













