Subscribe to get full access to this operation and the extensive Spine Surgery Atlas.
FREE TRIAL
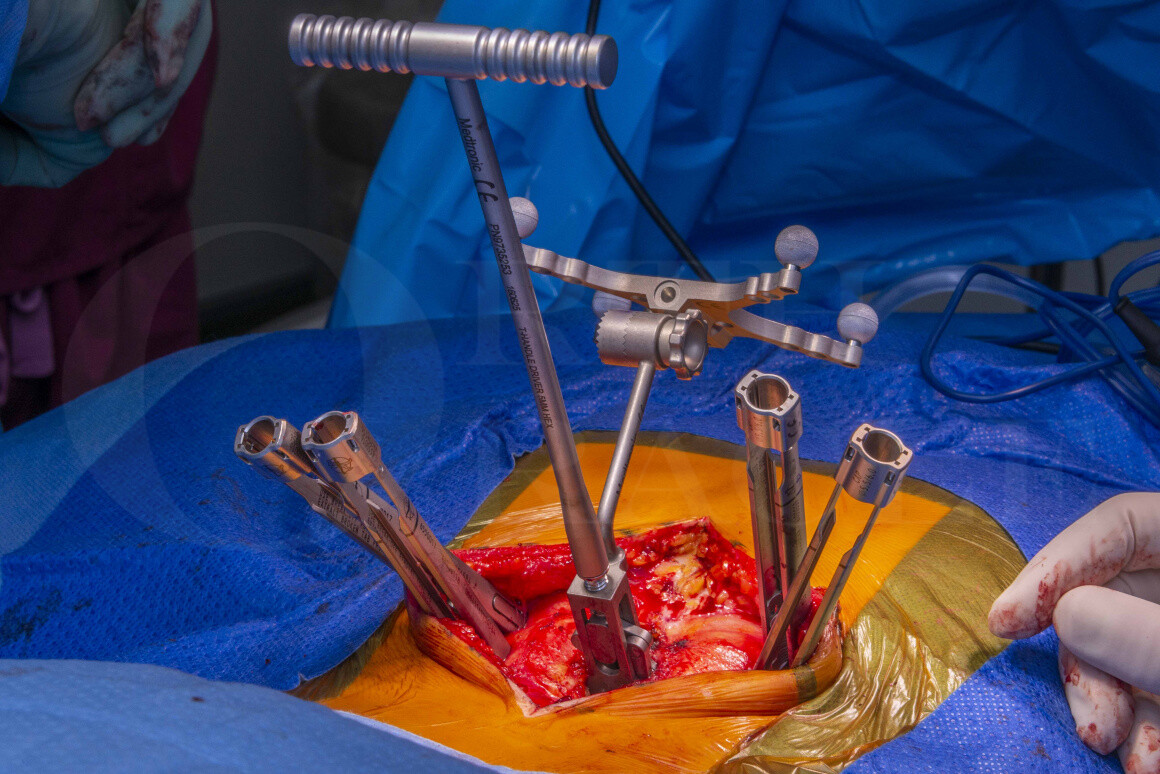
Learn the Hybrid Open/Minimally Invasive Navigated L5/S1 Transforaminal Lumbar Interbody Fusion (Medtronic CD Horizon Solera Voyager) surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Hybrid Open/Minimally Invasive Navigated L5/S1 Transforaminal Lumbar Interbody Fusion (Medtronic CD Horizon Solera Voyager) surgical procedure.
Degenerative disease affecting the lumbar spine is the commonest cause of spinal problems in the developed world. This is caused by abnormal loading of the lumbar spine exacerbated by factors that include a sedentary lifestyle, poor posture and raised body mass indices. Although this is a function of the ageing spine, the condition is also seen in young patients. Causes are multifactorial with genetic predisposition likely in younger patients.
The degeneration begins in the intervertebral disc that becomes dehydrated and prone to annular tears, loss of height and disc prolapse. Disc degeneration subsequently leads to abnormal stresses affecting the supporting structures and the classical picture of facet joint and ligamentum flavum hypertrophy.
Further possible sequelae to degenerative disease is spondylolisthesis, which is a disturbance in the normal alignment of the spine with one vertebra shifted forwards or backwards on another.
Spinal stenosis is a circumferential compression of the cauda equina nerve roots in the canal by a combination of disc bulge at the front, facet joint hypertrophy at the sides and ligamentum flavum hypertrophy at the back.
There may also be an additional dynamic component to the compression if there is associated segmental instability and spondylolisthesis.
Patients present with neurogenic claudication. This manifests as sensory disturbance and aching in the legs on exertion, so that their exercise tolerance becomes limited. They may also have radicular type leg pain, and in advanced cases they may have problems with bladder and bowel function and altered perineal sensation.
There are conservative and surgical treatment options for patients with severe lumbar canal stenosis. Surgical treatment is a decompression, which may need to be augmented with a fixation of there is evidence of underlying instability or if the decompression is likely to cause instability.
In this procedure I have achieved a 360 degree fixation at the L5-S1 level with navigated pedicle screws from the back and an interbody cage at the front.
Interbody cages can be introduced from posterior (posterior lumbar inter body fusion-PLIF) or posterolaterally (transforaminal lumbar interbody fusion- TLIF). PLIF cages tend to be smaller and require more retraction of neural structures for insertion. TLIF cages tend to be larger, and require less retraction.
There are a variety of TLIF cages on the market. Static cages can be placed obliquely spanning the disc space, or can be ‘turned’ inside the disc space to lie transversely at the front of the disc space. This second type are known as banana cages. They have the advantage of allowing the surgeon to create more lordosis at that segment with subsequent compression on the screw rod construct to hinge on the inter body cage. This is the cage that I am using in this technique.
A further evolution in cage design is the development of expandable cages. These can be expanded in the disc space in a controlled way. This has the advantage of minimising the passage of cage trials across the neural structures into the disc space, and may also allow for greater disc space distraction.
3D printed titanium cages have the advantage of a porous scaffold structure that promotes bony ingrowth and may lead to increased fusion rates. There are also favourable biomechanics properties with this cage with less stiffness than a conventional titanium cage.
I have used a hybrid open/minimally invasive approach. The open approach allows for a central lumbar decompression. The minimally invasive (MIS) approach reduces the need for far lateral exposure of the spine, and thus avoids significant paraspinal muscle stripping. The rationale for a hybrid strategy is to combine these benefits in a way in which the final endpoints are not compromised (decompression and fusion), whilst the invasiveness of the procedure is reduced. This translates into less post operative pain, more rapid mobilisation on the wards and shorter hospital stays, and lower infection rates.
Readers will also find the following OrthOracle instructional surgical techniques of interest:
Minimally Invasive Transforaminal Lumbar L5/S1 Interbody Fusion using Nuvasive pedicle screws, MAS retractor and Stryker OIC PEEK cage.
L4-S1 navigated transforaminal lumbar interbody fusion and decompression using Medtronic Solera and Artic-L
Minimally invasive posterior lumbar spine fusion (MidLIF) and decompression for spondylolisthesis with spinal stenosis (Medtronic Solera and Artic-L cage)
eXtreme Lateral Interbody Fusion (XLIF) – Nuvasive
Author: Mark Nowell FRCS
Institution: Southmead Hospital, Bristol, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu