Subscribe to get full access to this operation and the extensive Shoulder & Elbow Surgery Atlas.
FREE TRIAL
Learn the Open repair of subscapularis and biceps tenodesis, using Arthrex Bio-Swivelock anchors and TightRope button surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Open repair of subscapularis and biceps tenodesis, using Arthrex Bio-Swivelock anchors and TightRope button surgical procedure.
Rotator cuff tears are a relatively common cause of shoulder pain from the subacromial space. Supraspinatus, the elevator, is the most commonly effected tendon which then extends posteriorly into the adjoining infraspinatus, the external rotator. Subscapularis, the internal rotator anteriorly, is the least affected rotator cuff tendon. Rotator cuff disease that results in tears can be thought of as resulting from either intrinsic or extrinsic factors, or a combination of the two.
Intrinsic disease occurs due to a patient’s biological and genetic makeup, resulting in disorganisation of the collagen within the tendon, which degenerates and detaches from its bony footprint on the proximal humerus. Extrinsic causes are thought to be attritional wear from repetitive rotation and movement against a thickened coracoacromial ligament or subacromial bony spur. In the case of subscapularis anteriorly it may abrade against the underside of the coracoid process, resulting in rupture of the rotator cuff tendon attachment to the proximal humerus. Rotator cuff tears can also come about as a result of direct injury, with a fall or wrenching force to the joint or even a direct blow to the shoulder. This is the most common cause of a subscapularis avulsion tear when the shoulder is forced into external rotation whilst contracting to internally rotate.
Rotator cuff tears can be further categorised as either partial thickness or full thickness tears. The latter is a complete deficit of the tendon with detachment from the bone whereas the former describes fraying and scuffing of the upper (bursal) aspect or under (articular surface) aspect of the tendon. There may also be an element of intrinsic intra-substance change within the tendon structure which may only be apparent on cross-sectional imaging such as MRI scan.
Much has been published in the orthopaedic literature concerning the management of rotator cuff disease, and despite this its management is controversial with fervent supporters of both conservative and surgical treatment. Many shoulder surgeons though will advocate surgical repair of a torn or detached tendon once conservative measures have been proven to be unsuccessful. Exact surgical technique varies with surgeons’ preference, experience and ability and there is little evidence to suggest that the different described surgical techniques have widely different surgical outcomes.
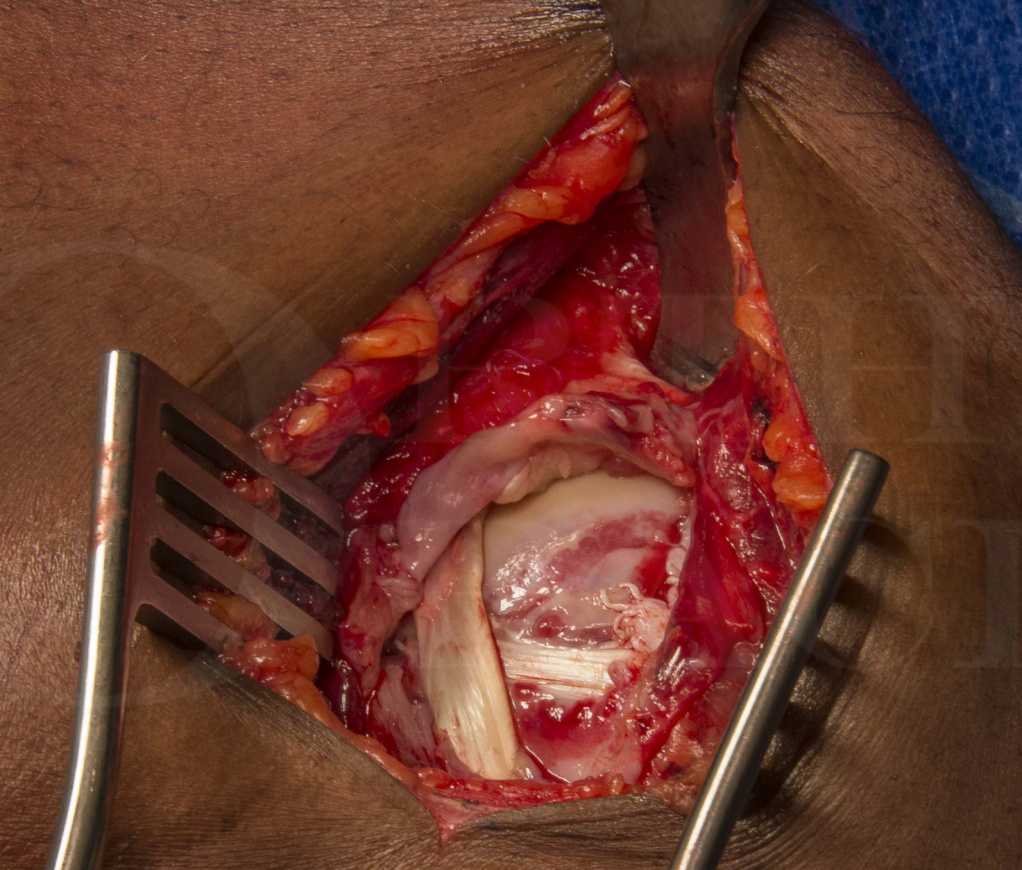
The technique described here is the one I use for an isolated full thickness tear of subscapularis with dislocation of the long head of biceps tendon out of the bicipital groove and ‘cheese-wiring’ over the top and front of the subscapularis tendon.
I use the Arthrex shoulder repair instruments and implants during these cases. As with much of the Arthrex inventory the system has been designed to make operations easier, by engineers and surgeons collaborating to optimise the solution. The set of instruments “covers all bases” in terms of having something that helps in every situation and the range of implants allows flexibility between types and sizes of anchors and suture material. In this case I use the 4.75 and 5.5 BioSwivelock C anchors with FiberTape suture material and the Arthrex TightRope implant for the biceps tenodesis.
Readers will also find of interest the following related OrthOracle techniques:
Arthroscopic subacromial decompression
Arthroscopic rotator cuff repair using modified Arthrex suture-bridge technique
Arthroscopic subscapularis tendon repair utilising Smith and Nephew Healicoils
Arthroscopic rotator cuff repair with Arthrex Speedbridge
Author: Mr Mark Crowther FRCS
Institution: The Avon Orthopaedic centre, Southmead Hospital, Bristol, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu