Subscribe to get full access to this operation and the extensive Upper Limb & Hand Surgery Atlas.
FREE TRIAL
Learn the Radial nerve exploration and nerve grafting using autologous graft and AxoGen AVANCE nerve allograft surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Radial nerve exploration and nerve grafting using autologous graft and AxoGen AVANCE nerve allograft surgical procedure.
The radial nerve is vulnerable to injury as it courses around the humerus in the spiral groove. Most radial nerve injuries associated with low energy fractures are of a low-grade, typically a neurapraxia with some degree of demyelination affecting the large myelinated fibres (prolonged conduction block) or with some partial and minor axon disruption (mixed nerve injury). These injuries usually recover fully in 6-12 weeks without surgical intervention for the nerve injury. Delayed recovery may necessitate exploration and decompression at the lateral inter-muscular septum.
One should be cautious when making such a diagnosis in the setting of a high energy injury, when there is neuropathic pain or when there is deterioration after intervention. In a case with intact function then loss after closed reduction and casting, one should anticipate that the nerve has been caught in the fracture and urgent exploration is warranted. At best the nerve will be swollen with haematoma compression at the lateral septum and decompression will improve the situation and the chance of recovery. When the onset of palsy follows surgical intervention with ORIF one should assume that there has been a direct nerve injury. The mechanism may be traction, entrapment under a plate, direct injury with a drill or screw. There is little merit in waiting and typically the pre-operative assessment is inadequate to confirm that intra-operative nerve trauma has occurred and unnecessary delay ensues whilst neurophysiology is requested.
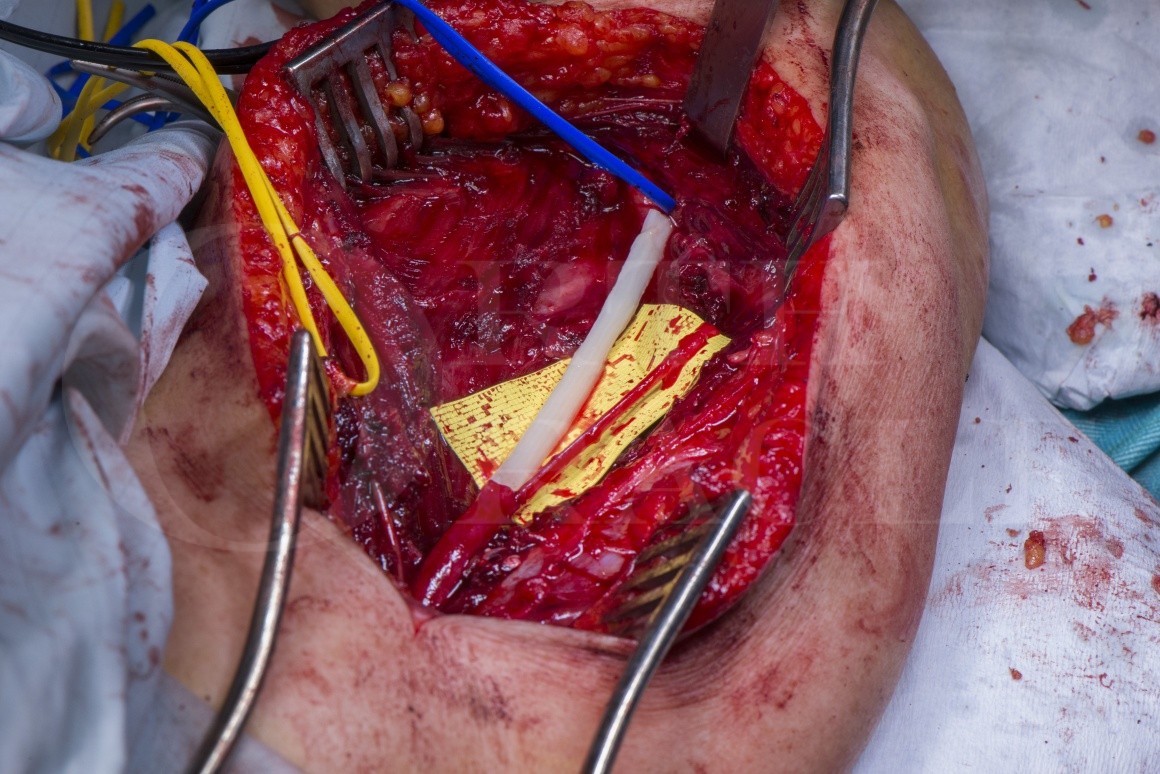
The case presented was referred to me at 8 months following fixation of a distal humeral fracture with a direct posterior approach and precontoured locking plates applied medially and posterolaterally to stabilise the fracture. Exploration confirmed injury to the radial nerve and the branch to brachioradialis from a drill bit with nerve rupture. A long gap of 7cm had resulted and the options for reconstruction are discussed.
An AVANCE processed nerve allograft was selected for the main radial nerve trunk as a pain management and sensory recovery strategy with autologous sensory nerve graft from the posterior cutaneous nerve of the forearm to the branch to brachioradialis. The case was combined with a distal pronator teres tendon transfer to the extensor carpi radialis brevis and nerves transfers from the median nerve to the posterior interosseus nerve for digit extension. This strategy was selected due to the timing of presentation and the low chance of any meaningful recovery through a long segment autologous graft at this stage.
Author: Dominic Power FRCS Orth, Consultant Hand and Peripheral Nerve Surgeon
Institution: Peripheral Nerve Injury Service, Queen Elizabeth Hospital, Birmingham, UK
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













