Subscribe to get full access to this operation and the extensive Spine Surgery Atlas.
FREE TRIAL
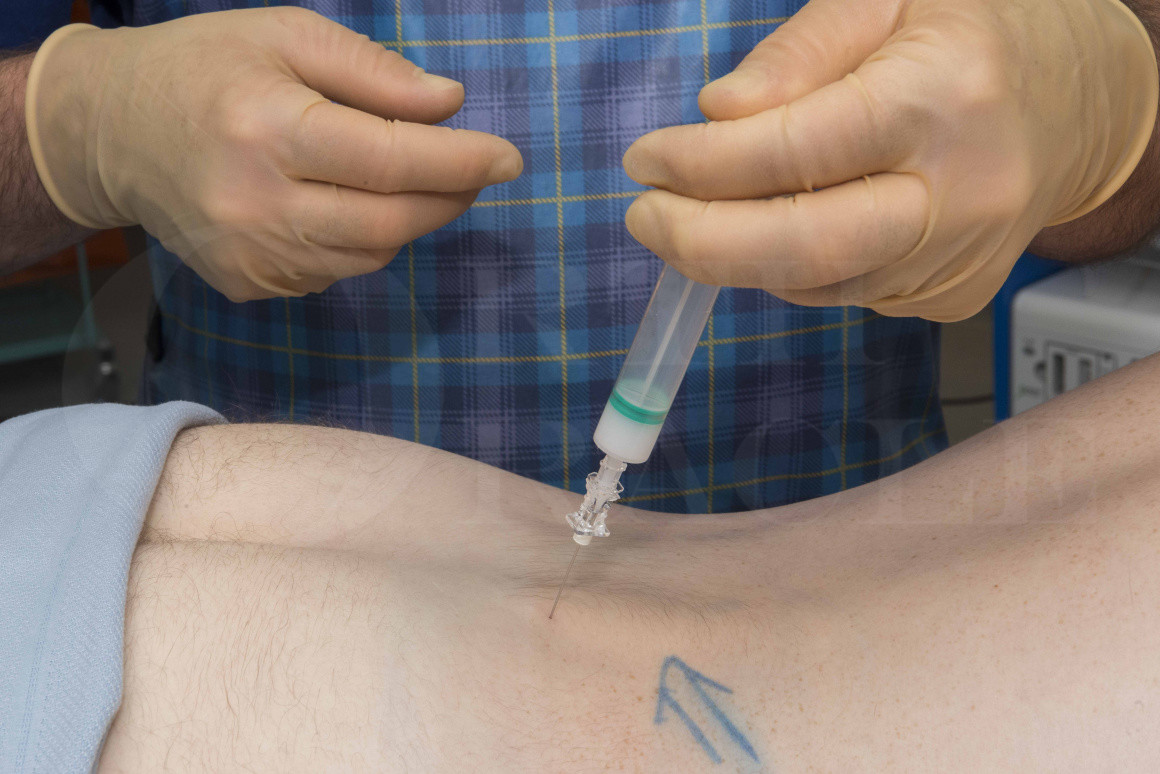
Learn the S1 Nerve Root injection using Image Intensification surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the S1 Nerve Root injection using Image Intensification surgical procedure.
Nerve root injection, or nerve block, is a very common procedure performed by spinal surgeons, pain physicians, and radiologists. It can provide excellent relief of severe neuropathic pain resulting from compression of an isolated nerve root.
A nerve root injection aims to deliver a combination of local anaesthetic and steroid into the epidural space around a nerve root. This allows a reduction in local inflammation which can improve the radicular pain associated with neural irritation. It can, therefore, be used to provide symptomatic relief from neuralgia caused by disc prolapse or spinal stenosis and can be placed around a nerve root at any level of the spine using fluoroscopic or CT-guidance. The lower lumbar and mid cervical spine have the highest prevalence of degenerative change and the L5/S1 disc is the most commonly affected by degenerative change so it is important to know how to inject around this area.
National guidance in the UK Low Back and Radicular Pain Pathway (https://ba17bc65-2f2f-4a2f-9427-cd68a3685f52.filesusr.com/ugd/dd7c8a_caf17c305a5f4321a6fca249dea75ebe.pdf) suggests a nerve root injection can be used to provide conservative measures for certain spinal conditions such as disc prolapse or spinal stenosis with radiculopathy; when used for patients who have a disc prolapse causing radiculopathy, up to 50% of patients will find they get good medium to long term relief of their symptoms. This is because the disc prolapse resorbs before the effect of the steroid wears off. However, for the remainder, the effect of the steroid wears off before the disc prolapse resolves so the neuralgia returns. In spinal stenosis, the underlying neural compression does not resolve over time and so the rate of long-term relief following a steroid injection may be lower compared to those used for a disc prolapse. Around 30-40% of patients will have good medium to long term improvement in pain. It is worth bearing in mind that it is effective in aiding radicular pain associated with spinal stenosis but not the spinal claudication aching which comes on when standing or walking.
The local anaesthetic lasts for a short time depending on which local anaesthetic is used and generally will last between one and six hours. The effect of the steroid tends to build up over the first 24-72 hours; a small proportion of patients will have a flare up of their pain for a few days but most find the pain disappears fairly quickly. If the pain does return, this can be anytime between a few days and a few months after the injection.
It can be performed with or without sedation depending on patient preference, but the majority find it acceptable to not have sedation. A phobia of needles or extreme pain on lying prone may be indications to use sedation.
Author: Mr Stephen Morris FRCS (Tr & Orth).
Institution: Avon Orthopaedic Centre, Southmead Hospital, Bristol
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu