Subscribe to get full access to this operation and the extensive Upper Limb & Hand Surgery Atlas.
FREE TRIAL
Learn the Ulnar corrective osteotomy: Distal periarticular osteotomy fixed with Synthes Hook plate surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Ulnar corrective osteotomy: Distal periarticular osteotomy fixed with Synthes Hook plate surgical procedure.
Distal ulna fractures are not rare, and are often unstable due to the rotational forces at the fracture site. They are commonly associated with distal radius fractures and are often comminuted and intra-articular due to the force required to fracture both bones. Therefore such ulnar fractures are usually treated operatively primarily, which minimises the risk of malunion occurring.
Ulnar fixation is usually performed at the time of surgery to the distal radius and can be with the ulna Hook plate, k-wires or other plating systems, depending on the fracture configuration. Distal ulna fractures usually go into extension with the distal radius but reduce when the radius is fixed. The rotation of the forearm however remains a deforming force meaning there can easily be a rotational malunion if an unstable ulna fracture is not stabilised. In addition, over time the brachialis muscle, inserting on the olecranon, will try and pull the ulna onto the radius, and without the ulna head to prevent it, the distal diaphysis with lean radially and push the ulna head fragment into ulnar deviation as occurred in this case.
Whether a malunion of these fractures needs intervention will depend on a patient’s symptoms, in most cases. If the rotational deformity is the main issue and if the patient can tolerate the loss of movement then lower demand and older patients may be adequately treated non-operatively. If the ulnar angulation of the fracture gives an ulnar positive wrist, as in this case, then impingement on the lunate may cause a pain issue, requiring surgery. Finally if there is an extension or flexion deformity then the severity of symptoms will be relative to the depth of the sigmoid notch accommodating the ulna head. The flatter the notch, the more forgiving the joint is to this type of malunion.
The need for an osteotomy is not common at this location on the ulna however the Hook plate plate is regularly used in the treatment of ulna styloid fractures.
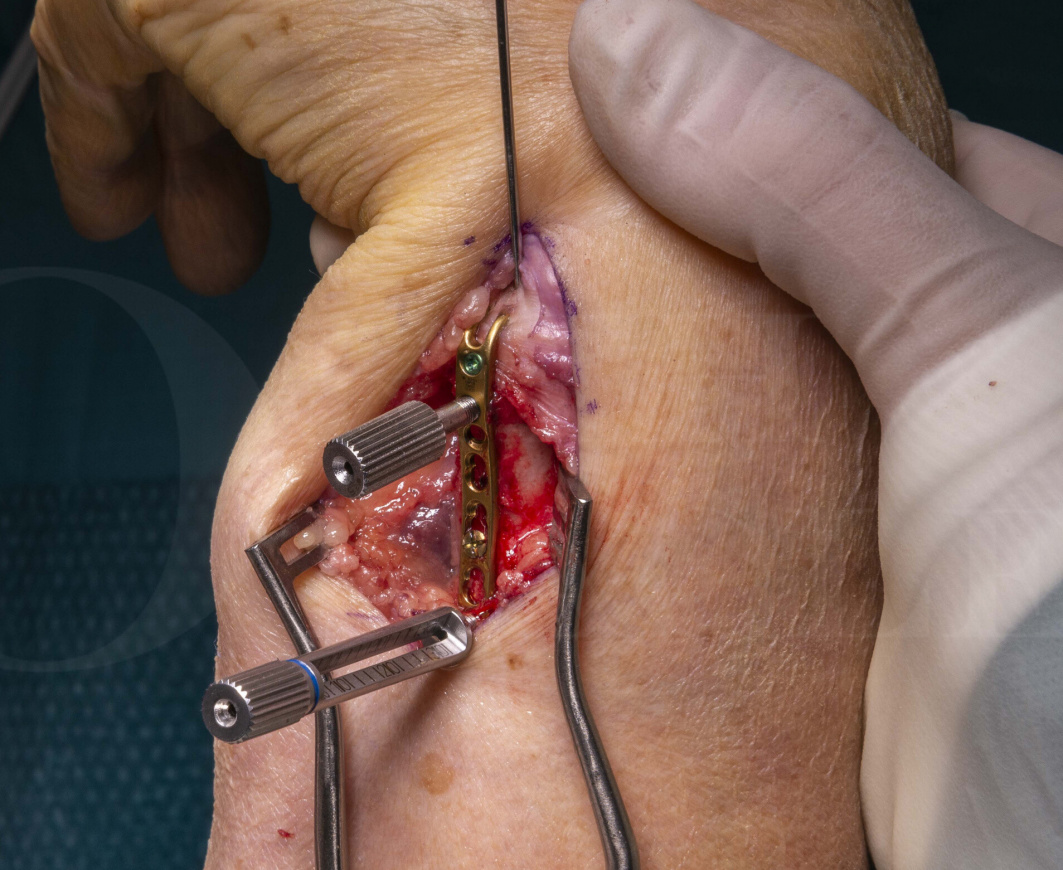
The main advantage of the Ulna Hook plate catching over the tip of the ulnar styloid is to aid in reduction and provide an immediate and easily adjustable anchor point to stabilise the distal fragment. There is a potential disadvantage that its prongs may cause soft tissue issues. If placed beneath the extensor retinaculum and on the styloid tip, then the plate does not tether or impinge to any notable level.
The Ulna Hook plate has the potential for locking screws along its whole length and non-locking screws in the diaphyseal section. A single oval hole to allow minor plate adjustment after the primary screw insertion is also present. The plate comes in stainless steel however other manufacturers do offer a titanium version with a similar design.
In the context of a corrective ulna osteotomy non-union is a concern due to the poor quality of the bone in these patients (who tend to be older), poor vascularity of the neck and diaphysis of the ulna and also the rotational deforming forces at the osteotomy site. This is therefore the rationale for having the patient in a cast that stops forearm rotation for 8-12 weeks and confirming the union with a CT scan if there are any concerns.
Author: Mark Brewster FRCS(Tr & Orth)
Institution: The Royal Orthopaedic Hospital, Birmingham, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













