Subscribe to get full access to this operation and the extensive Shoulder & Elbow Surgery Atlas.
FREE TRIAL
Learn the Distal Humeral fracture(Hoffa type): Internal fixation with Medartis plate surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Distal Humeral fracture(Hoffa type): Internal fixation with Medartis plate surgical procedure.
Distal humerus fractures account for approximately 10% % of the overall incidence of fractures in the adult population and have seen an increase of 9% during the last decade. Overall the majority occur in females and there is a double peak in age distribution, with the first peak is between the 20 and 30 where males are in the majority, female patients in the second peak, over 70 years, predominate.
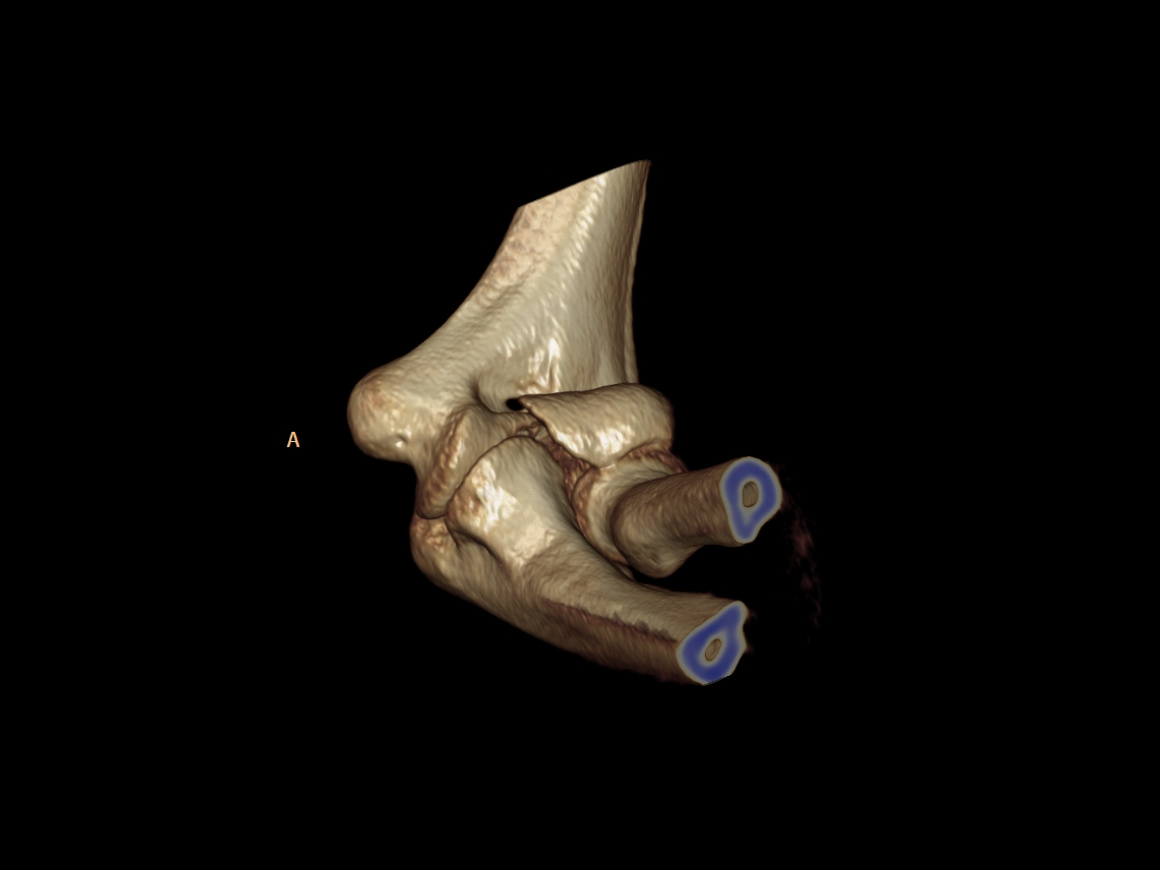
Capitellar fractures with an intra-articular split in the coronal plane are called Hoffa type fractures named after Albert Hoffa, a German orthopaedic surgeon, innovator, and professor of Orthopaedics in Berlin at the start of the twentieth century.
The AO classifies these fractures as 13B3; these B3 type fractures are further subclassified by Dubberly in 1, 2 or 3 regarding how far the fracture line is ulnar and into A/B with respect of the posterior column.
Hoffa type fractures mostly result from direct high energy trauma, which cause a shear force on the anterior capitellum. In the younger population there tends to be little fracture comminution with these fractures, whereas comminution can prove a challenge to reconstruction in older patient with osteoporotic bone.
The elbow joint is very intolerant of any articular surface incongruity, so anatomical reconstruction must be the aim with all these fractures. Moreover, since the nutrition of the anterior capitellum is provided only from the bony proximal humerus a displaced Hoffa type fracture fragment is at substantial risk of avascular necrosis and its reduction is an urgent surgical priority, and certainly should not be delayed more than 24 hours at very most.
These fractures are also particularly prone to subsequent complications such as elbow stiffness, post-traumatic arthritis and heterotopic ossification of the soft tissue, so the early mobilisation that stable internal fixation permits should be an aim as often as possible.
Open reduction and internal fixation is the main approach used to treat displaced capitellar fractures and its objective is to reconstruct the capitellum anatomically which minimises the chance of articular degeneration and avascular necrosis, with primary stability following surgery allowing early functional postoperative training to prevent elbow stiffness.
There has been some discussion in the literature about the optimal surgical approach for these fractures, with anterior approaches being favoured in the paediatric population and lateral or posterior lateral approaches being most commonly used in the adult.
There are some surgeons who advocate trans-articular screw fixation, but whatever the screw design this produces further articular surface damage. There is however far more literature that advocates, as do I, fixation from lateral or posterior approach using screws or locking plates, which avoids direct transgression of the articular surface.
The Medartis elbow radial plate has been intelligently designed to assist the surgical management of distal humeral fractures. It has several advantages for this fracture type, in particular, its anatomic pre-contour supports fracture reduction and the options fit the distal humerus well, its low profile design reduces soft tissue problems, and the screw holes are well positioned and allow flexibility, with a centrally placed long hole for lag screw fixation and easy fine tuning of the plate position, and multidirectional locking options for poly-axial locking screws which allows 15° from perpendicular variability of screw placement, which is very helpful in these often comminuted fractures. Also all screw holes accept either classical cortical screws or locking screws with a diameter of 2.8mm. There is a radial extension limb to the place allows for additional screw fixation at 90 degrees to the main plate fixation, into the distal articular fragments which is of great assistance with comminuted fractures.
OrthOracle readers will also find the following related instructional operative techniques of interest:
Humeral fracture: Transcondylar distal fracture fixation with Synthes 2.7mm/3.5mm Variable Angle Locking Compression Plate, triceps sparing approach
Humeral fracture: K-wiring of Supracondylar flexion pattern fracture.Humeral fracture: Transcondylar distal fracture fixation with Synthes 2.7mm/3.5mm
Humeral fracture: Fixation of distal third fracture using Synthes LCP extra-articular distal humeral plate
Radial Head Fracture: Open Reduction and Internal Fixation with Medartis 3.0mm CCS Screws and LUCL repair using Arthrex Biocorkscrew anchor
Radial Head Replacement Using Evolve Proline Modular Radial Head System (Wright Medical)
Olecranon fracture : Suture tension-band fixation using Arthrex Fibretape sutures
Olecranon fracture: Fixation with Synthes LCP Olecranon plate
Author: Professor Peter Biberthaler, MD.
Institution: Technical University of Munich, Klinikum rechts der Isar,Munich, Germany.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













