Subscribe to get full access to this operation and the extensive Foot Surgery Atlas.
FREE TRIAL
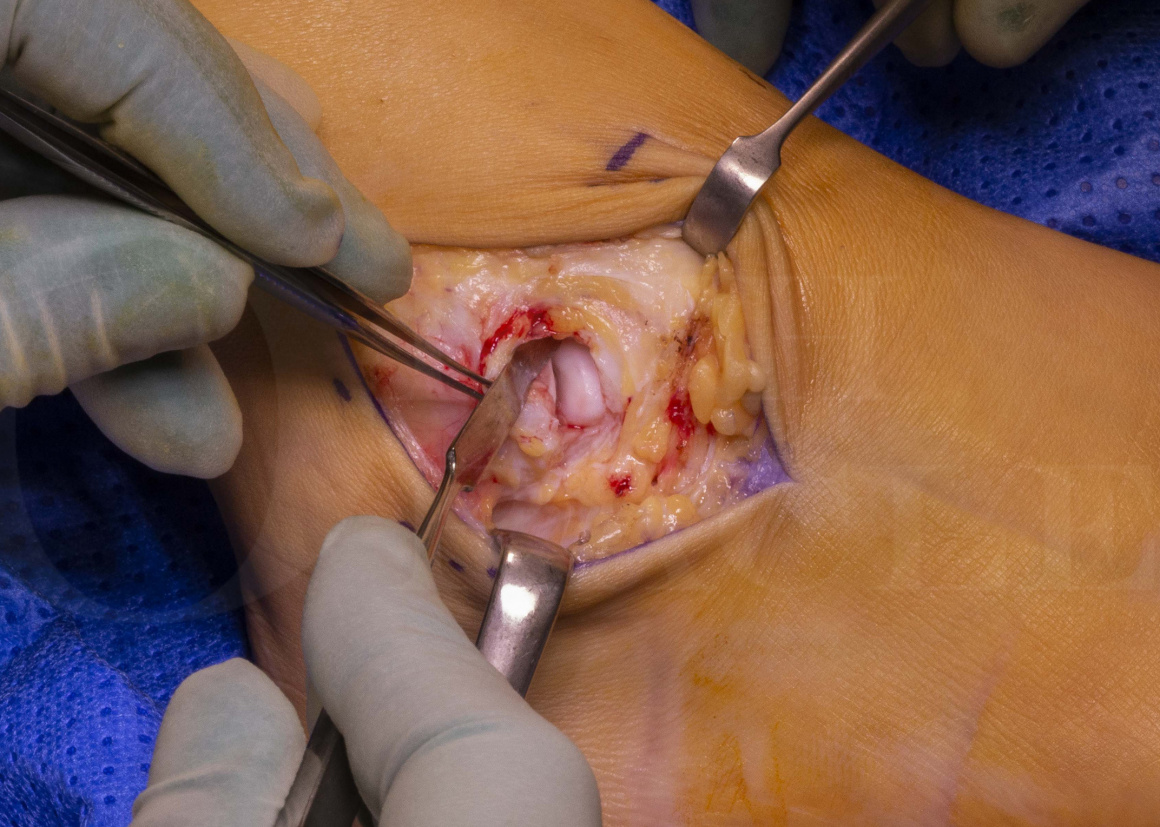
Learn the Lateral ankle ligament reconstruction: Broström (mid-substance) repair surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Lateral ankle ligament reconstruction: Broström (mid-substance) repair surgical procedure.
Chronic ankle instability is a potential sequel to acute ankle sprains and refers to persistent giving way of the ankle. There are a number of causes of ankle instability including structural instability, functional instability and pseudo-instability. Functional instability describes an instability that is secondary to a proprioceptive deficit Functional instability is most effectively addressed with an appropriate physiotherapy lead rehabilitation programme, to restore proprioception and coordination. Pseudo-instability is a feeling of instability in the ankle; In pseudo-instability the ankle usually doesn’t give way completely, individuals are often able to protect the ankle before it gives way and they might complain of a consistent feeling of catching or discomfort prior to the ankle giving. Pseudo-instability is usually caused by pain generators such as loose bodies or osteochondral lesions of the ankle.
Structural instability refers to an instability that is secondary to laxity of the ankle ligaments, usually the anterior talo-fibular (ATFL) and the calcaneo-fibular ligament(CFL). Structural instability is characterised by an increased excursion of the talus relative to the ankle mortise. At initial presentation, many patients with structural instability will have a degree of functional instability as well. The functional element of instability should be addressed with a course of functional rehabilitation with a physiotherapist before addressing the structural element. Even patients with significant structural instability may compensate satisfactorily by improving the functional component of their instability.
Those patients with persistent structural instability, despite adequate physiotherapy, may benefit from surgery to stabilise the ankle, which aims to address the structural component by repairing or re-constructing the ATFL and CFL.
One surgical technique that provides excellent results was first described by Brostrom in 1966, whereby the ATFL and CFL are repaired under tension. Gould in 1980 described a modification, incorporating an additional imbrication of the inferior extensor retinaculum (IER). The Bröstrom-Gould technique forms the mainstay of anatomic ankle reconstruction techniques, not only because of the high success rates, but also because of low rates of complication, such as ankle stiffness, subtalar arthritis and nerve injury. The procedure also restores the normal kinematics of the joint. Unlike the anatomical repair, non anatomical reconstructions(such as the Chrisman-Snook or Evans procedure) may not restore normal kinematics of the joint and usually involve larger dissections with a higher complication rate, most notably nerve injury and subtalar stiffness.
Readers will also find the following OrthOracle surgical techniques of interest:
Brostrom lateral ligament reconstruction using JuggerKnot soft tissue anchor(Zimmer-Biomet).
Lateral ankle ligament reconstruction
Ankle arthroscopy using the Smith and Nephew Guhl non-invasive ankle distractor
Peroneal sheath reconstruction (for peroneal tendon subluxation)
Author: Nick Cullen FRCS (Tr & Orth)
Institution: The Royal National Orthopaedic Hospital, Stanmore, London, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













