Subscribe to get full access to this operation and the extensive Bone & Soft Tissue Tumour Surgery Atlas.
FREE TRIAL
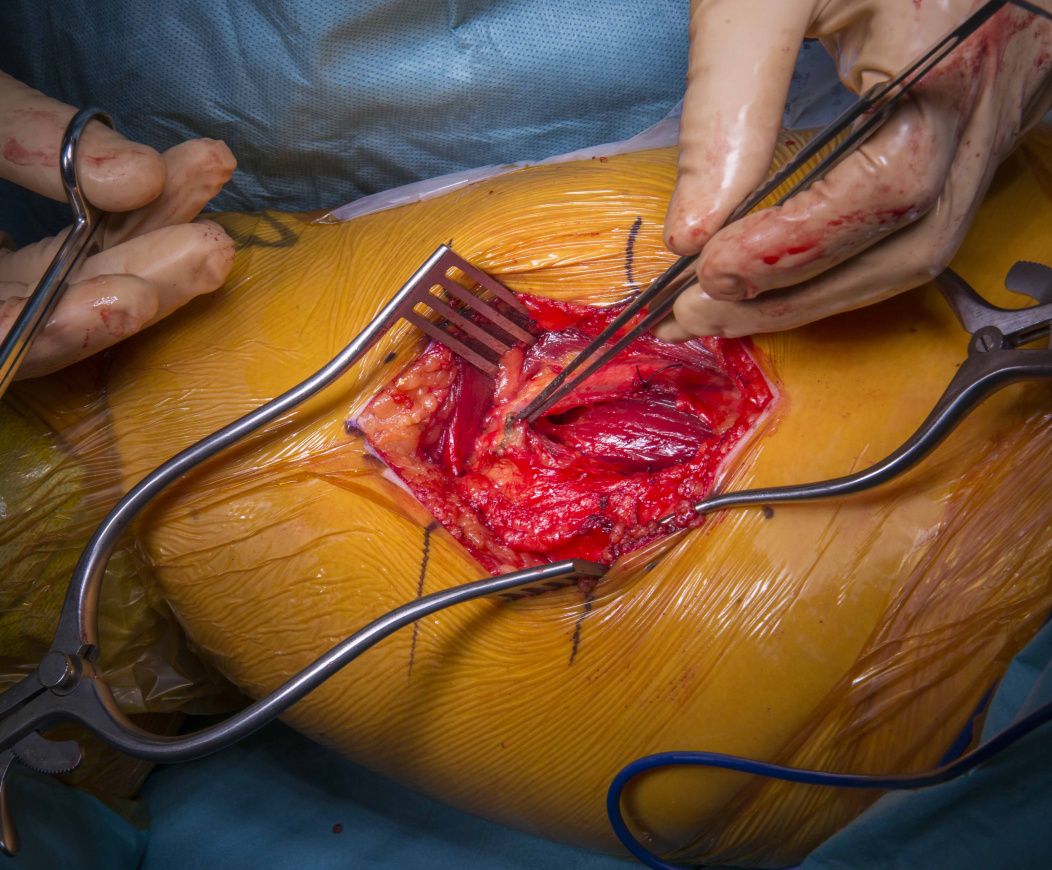
Learn the Excision of myxoma from Hunters canal( medial thigh) surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Excision of myxoma from Hunters canal( medial thigh) surgical procedure.
In the WHO Classification of Tumours of Soft Tissue and Bone, myxomas are included in the section headed ‘Tumours of uncertain differentiation’. There are four main sub-types: acral fibromyxoma; intramuscular myxoma; juxta-articular myxoma; deep (aggressive) angiomyxoma. Of note myxoma may also occur in the heart or the eye. The most common sub-type encountered by the orthopaedic surgeon is the intramuscular myxoma. Patients present with a lump which may or may not be painful. Ultrasound scanning followed by MRI is recommended for investigation. Most centres dealing with soft tissue and bone tumours would recommend biopsy to confirm the diagnosis. A discussion can then ensue with the patient regarding excision if symptomatic. The main risks of excision include wound problems, infection, damage to adjacent critical structures and recurrence.
Intramucular myxomas are benign tumours of mesenchymal origin. The incidence is 1 in 1 million with a slight female preponderance of 57%. The typical age range of presentation is 40-70 years. 64% of patients will notice an enlarging mass, with the rest being incidental finding. 55% report that the tumour is painful. The size on presentation ranges from 1-17cm. They can be solitary or multiple. If they are multiple then the patient should be investigated for Mazabraud syndrome which features monostotic or polyostotic fibrous dysplasia.
It is important to note that if there is any doubt about the diagnosis, a biopsy must be performed to rule out a malignant tumour. There are no reports of malignant transformation of intramuscular myxomas. Therefore if the patient has none or minimal symptoms, non-operative management is recommended. If the patient is symptomatic then excision can be performed. Risks include damage to adjacent critical structures such as large nerve or blood vessels, wound problems, infection and recurrence rates of 30% at a median of 8.5 years.
Author: Mr Kenny Rankin FRCS (Tr & Orth)
Institution: The Freeman Hospital, Newcastle, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













