Subscribe to get full access to this operation and the extensive Spine Surgery Atlas.
FREE TRIAL
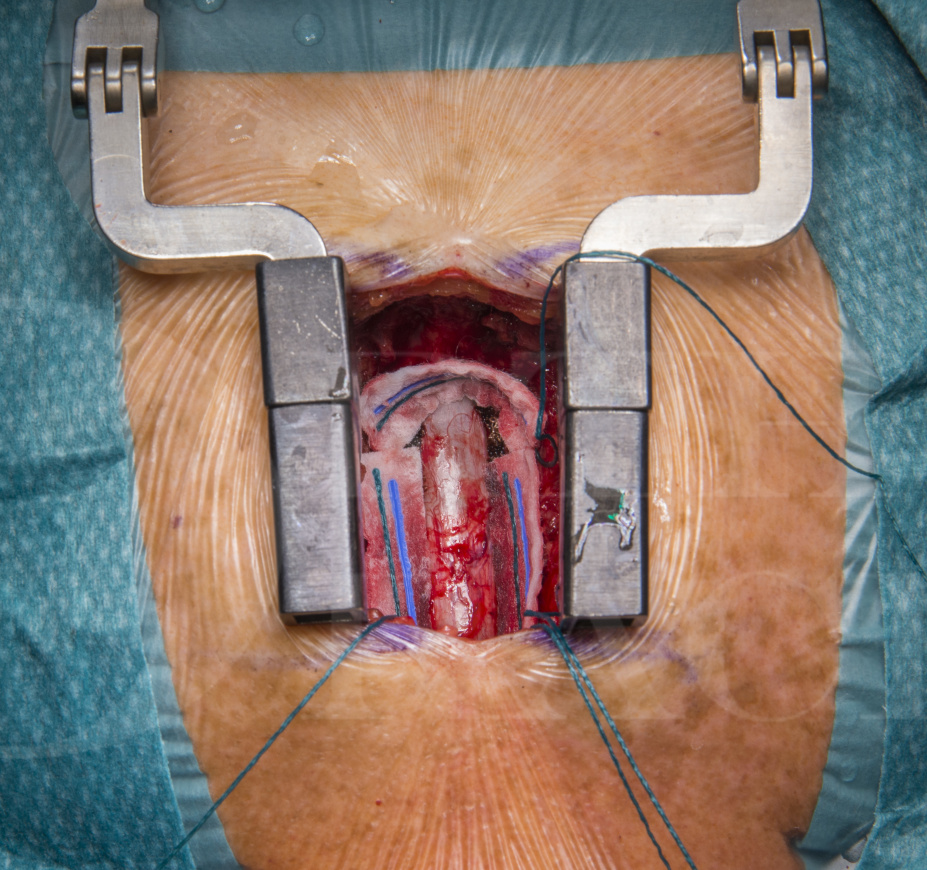
Learn the T1/2 Posterior Thoracic Laminoplasty( fixation with DePuy Synthes Matrix Neuro mini-plates) and excision of an intradural tumour surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the T1/2 Posterior Thoracic Laminoplasty( fixation with DePuy Synthes Matrix Neuro mini-plates) and excision of an intradural tumour surgical procedure.
Spinal tumours are generally rare and can be classified into:
- Extradural tumours
- Intradural extramedullary tumours
- Intradural intramedullary tumours
The case described involves a patient with Neurofibromatosis Type 2 with an intradural extramedullary tumour in the upper thoracic spine at the T1/T2 level.
Neurofibromatosis Type 2 (NF2) is a rare genetic condition which can be inherited as an autosomal dominant pattern. It is caused by a mutation in the NF2 gene which regulates the production of a protein called merlin/schwannomin which is a tumour suppressor protein. NF2 patients can develop benign fibrous tumours of the skin (cutaneous neurofibromas), bilateral vestibular schwannomas, meningiomas and gliomas. Bilateral vestibular schwannomas are diagnostic of NF2. The incidence is approximately 1 in 33000.
The clinical presentation will depend on the location of the tumour and typically if there is a lesion causing compression of the spinal cord or nerve roots then surgery is indicated. Spinal nerve sheath tumours are most often benign but in very rare cases can transform into malignant tumours.
The operating surgeon will need to assess the location of the tumour in relation the spinal cord in order to decide on the safest surgical approach. In principle, the technique used should keep manipulation of the spinal cord to the minimum with a view to mobilising tumour away from critical structures and into a ‘safer’ zone. Internal debulking of the tumour mass is also utilised to facilitate tumour mobilisation and removal. Sacrificing a nerve root can be considered if the aim is for tumour excision and the potential neurological deficit is not seen as being significant. The surgical strategy and risk of post-operative neurological deficits needs to be discussed with the patient prior to surgery.
Author: Navin Furtado FRCS.
Institution: The Queen Elizabeth Hospital, Birmingham, UK
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













