Subscribe to get full access to this operation and the extensive Upper Limb & Hand Surgery Atlas.
FREE TRIAL
Learn the Targeted muscle re-innervation for superficial radial neuroma surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Targeted muscle re-innervation for superficial radial neuroma surgical procedure.
Targeted muscle reinnervation (TMR) is a technique developed for the management of symptomatic neuromas. The ideal method of management for a neuroma is not clear. Different techniques may be required for different nerves in different locations. As a general rule though, reconstruction of the nerve gap created after resection of a neuroma is the optimum method of restoring some afferent signalling to the sensory cortex of the brain. Reconstructive procedures like this depend on the tissue bed, the quality of the distal nerve stump and the nerve gap.
Bridging a gap requires nerve graft and for some patients, the thought of creating a second nerve injury site for autologous nerve graft harvest, with the attendant risks of neuroma, sensory loss and neuropathic pain, is an unacceptable solution. TMR has demonstrated excellent results in the prevention of phantom pain, in the management of limb pain following amputation and in treating both mixed nerves and pure sensory nerves. The technique is “active” or reconstructive, directing regenerating axons into a distal motor branch of a nerve in the vicinity.
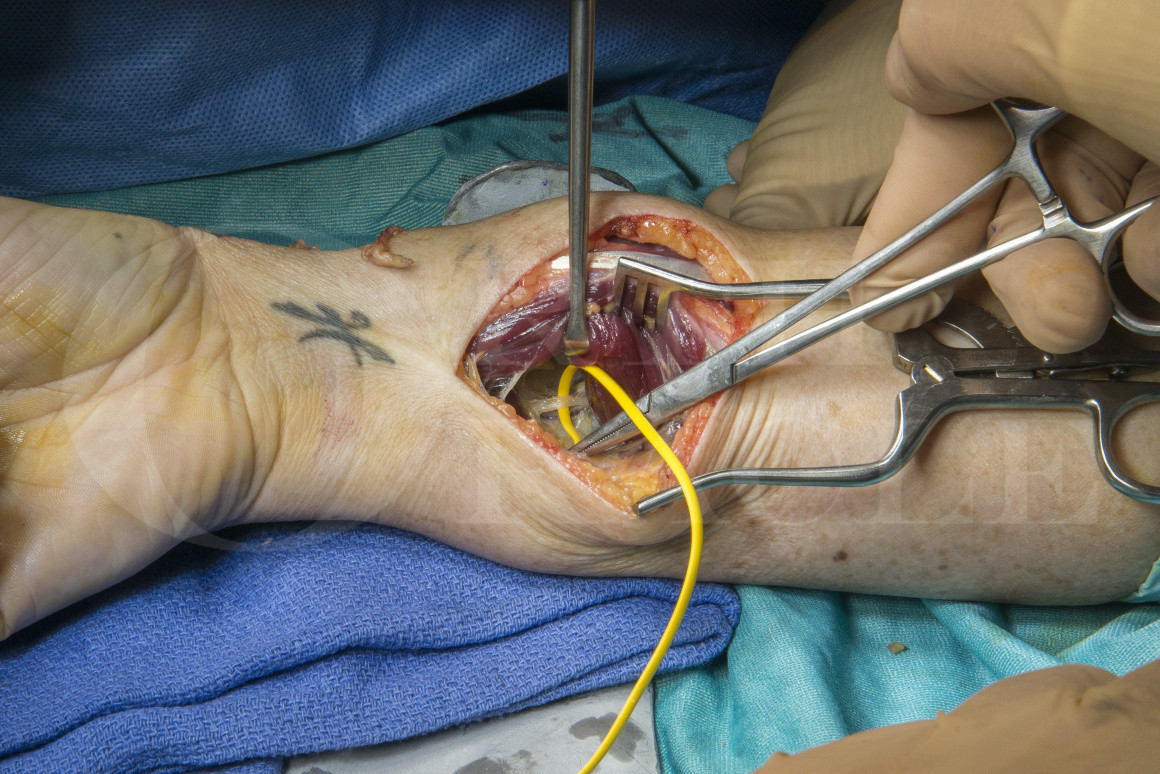
The superficial radial nerve is challenging to treat when sensitised, due to the prominent location and tendency fro irritation by contact from clothing. There is no wholly reliable method for management of the SRN. Applying the technique of TMR to the SRN is starting to demonstrate promise.
This technique demonstrates the use of TMR to treat a SRN proximal stump to the distal anterior interosseous nerve (AIN) to pronator quadratus (PQ) for the management of neuroma pain that followed injury to the SRN during injection to the thumb CMCJ. The initial attempts at neuroma management included in situ capping and relief was temporary, again becoming problematic at 2 years and being accompanied by CMCJ deterioration, in this case with pre-existing arthritis. Definitive treatment of the CMCJ arthritis with excision arthroplasty was planned and a decision to undertake TMR of the SRN at the same time was based on an attempt to find a more permanent resolution of the neuropathic pain.
Author: Dominic Power MA MB BChir FRCS FRCS Tr & Orth
Institution: Consultant Hand and Peripheral Nerve Surgeon
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













