Subscribe to get full access to this operation and the extensive Bone & Soft Tissue Tumour Surgery Atlas.
FREE TRIAL
Professional Guidelines Included
Learn the Total Hip Replacement: Implantcast PRS cup cage and dual mobility reconstruction for pathological acetabular fracture surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Total Hip Replacement: Implantcast PRS cup cage and dual mobility reconstruction for pathological acetabular fracture surgical procedure.
Metastatic bone disease commonly presents to the orthopaedic surgeon, bone being the most common site of metastasis. For example approximately 60% to 70% of patients with breast cancer develop bone metastases during the course of their disease. Skeletal related events (SREs: pathological or impending fracture, hypercalcaemia, spinal cord compression, severe pain) may require surgery and/or radiotherapy to palliate pain and to maintain both the capacity to walk and quality of life.
Due to advances in management of common malignancies, particularly breast and prostate carcinoma, patient survival has been extended to the point that these are now considered chronic diseases rather than terminal diseases. Consequently, the prevalence of metastatic bone disease continues to escalate. In well selected cases surgery is advocated for bone metastases, for example those with favourable prognostic criteria such as positive hormone receptor status and no visceral metastases. Clearly most surgical procedures in this context are performed with palliative rather than curative intent and often patients have very poor prognoses, consequently the surgical strategy must balance the patient’s life expectancy which requires thorough staging of the extent of metastatic burden and inclusion of oncologists to estimate. For patients with metastatic bone disease presenting to orthopaedic surgeons, and who undergo surgery, the median life expectancy is thought to be 12 months according to Raschka et al.
Peri-acetabular metastases with impending or completed pathological fractures are amongst the most challenging situations of surgeons and patients. Bone destruction and loss of anatomical landmarks combined with a palliative patient combine to create a high risk surgical procedure with limited time for pre-operative modification of any co-morbidities due to clinical urgency. Similarly, due to the acute presentation of these cases, time is limited to plan and manufacture custom 3D printed hemipelvic replacements which could be obsolete in the time taken to obtain such custom prostheses due to progressive bone loss due to tumour and fracture. Furthermore the clinical risks of lying in bed with a pathological pelvic fracture (such as thrombus, chest infection, bed sores), not to mention the cost for a custom prosthesis are not insignificant. Therefore an ‘off-the-shelf’ modular acetabular reconstruction system that can cope with severe acetabular bone loss has huge advantages.
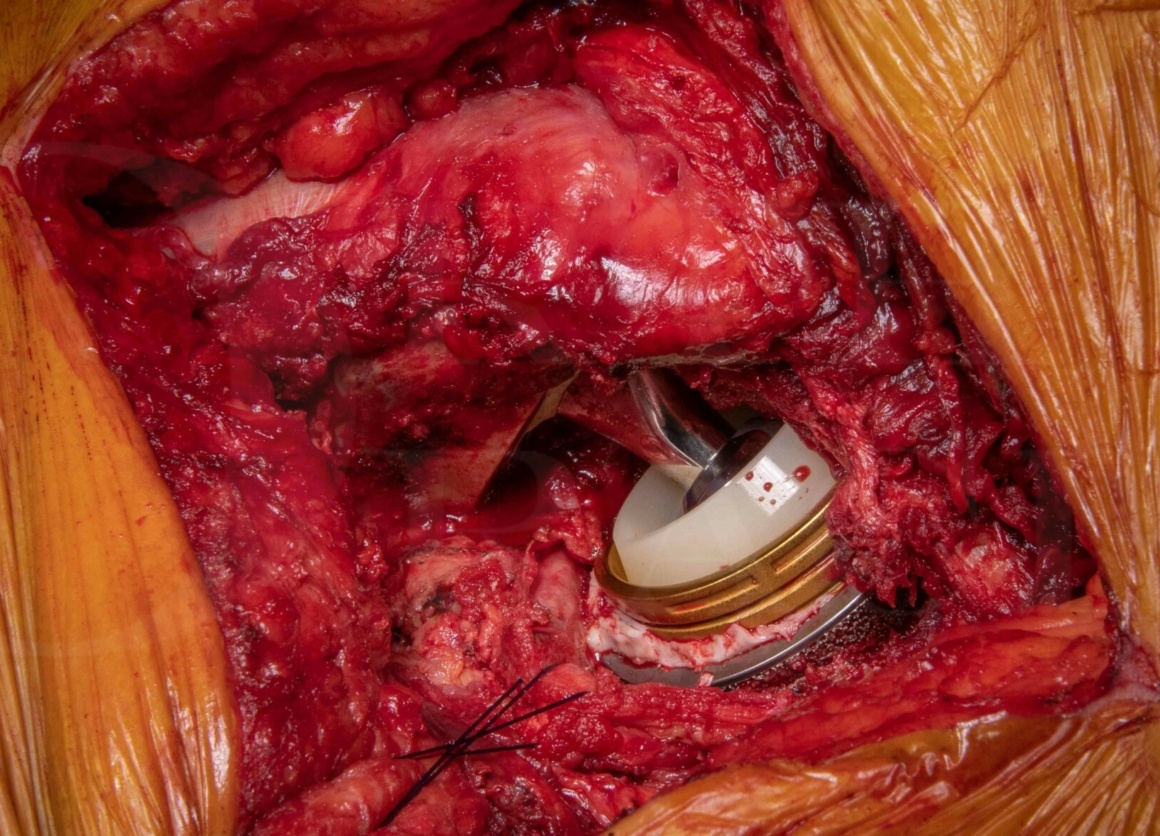
In this case I describe the use of the Implantcast PRS cementless hemispherical pelvic reconstruction cage and complex primary hip replacement for an impending pathological acetabular fracture and central dislocation due to metastatic thyroid carcinoma after pre-operative embolisation.
This type of implant is utilised in orthopaedic oncology (and acetabular trauma an drevision arthroplasty) up to Paprosky 3a defects to reconstruct the peri-acetabulum due to bone loss due to tumour involvement. Pelvic anchoring is provided by porous cage combined with an 8mm x 70-100mm cancellous screw into the ilioschial bar to achieve a stable acetabular reconstruction. Having reconstructed the acetabulum, an acetabular cup is cemented into the cage for use with a femoral prosthesis of your choice. Recent evidence has confirmed that dual-mobility articulations reduce the risk of dislocation with hemi-pelvic endoprostheses, so this case describes the use of a cemented dual-mobility acetabular cup and bearing.
Readers will find the following OrthOracle instructional techniques also of interest:
Proximal femoral endoprosthesis: Adler Pantheon for reconstruction after radical excision of femoral metastasis and trochanteric reattachment using Kinamed SuperCables
Proximal femoral endoprosthesis: Revision of THR to Adler Pantheon for metastatic bone disease progression
Proximal femoral endoprosthesis: Stanmore METS implant (Stryker) with trochanteric reattachment for pathological fracture
Navigated coned hemi-pelvis endoprosthesis (Stanmore METS, Stryker) with dual mobility acetabulum (Avantage, Zimmer Biomet) and modular proximal femoral endoprosthetic replacement with trochanteric reattachment (Stanmore METS, Stryker)
Total Hip replacement(posterior approach): Exeter stem (Stryker) and Gap II restoration acetabular cage (Stryker) for acetabular metastases.
Author: Jonathan Stevenson FRCS (Tr & Orth)
Institution: The Royal Orthopaedic Hospital, Birmingham, UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













