Subscribe to get full access to this operation and the extensive Spine Surgery Atlas.
FREE TRIAL
Learn the Lengthening of Medtronic Early Onset growing rods for scoliosis surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Lengthening of Medtronic Early Onset growing rods for scoliosis surgical procedure.
Scoliosis is a rotational deformity of the spine resulting in a lateral curvature. If it occurs before a child is 10 years old, it is termed early onset scoliosis (EOS). This incorporates the traditional terms of infantile scoliosis in 0-3 yrs old age group and juvenile scoliosis in 3-10 yrs old, and reflects the different management principles required to treat it when compared to late onset scoliosis in older children.
It is an uncommon diagnosis with a prevalence of around 0.08%. An asymmetry in the spine, shoulder imbalance or sitting imbalance will normally be identified by the child’s carers or a healthcare professional. The underlying aetiology may be idiopathic (no specific cause) or can be related to neuromuscular conditions, syndromal scoliosis or congenital abnormalities. It is also associated with previous surgery involving the chest wall, such as for congenital cardiac disease. Once identified, it is monitored over the course of years for any progression, and treated accordingly. Treatment will depend on the location and magnitude of the curve, rate of progression, underlying aetiology, medical co-morbidities and the wishes of the patient and their family. Whilst most EOS curves are treated conservatively, some progressive curves will require plaster jacket, brace therapy or surgery.
The most common operation for scoliosis in older children is to perform a posterior scoliosis correction with fusion of the spine. However, in children with early onset scoliosis, the chest is still developing and performing a fusion operation could result in a smaller thoracic height which can be associated with respiratory impairment and risk of premature death; this is called thoracic insufficiency syndrome. Alveoli are known to develop until 7 yrs old, then hypertrophy thereafter. Maintaining chest wall compliance and maximising the thoracic height during this period of early growth must be balanced against controlling a progressive scoliosis in order to reduce long-term disability.
In order to allow ongoing growth whilst controlling the scoliosis, ‘growth-friendly’ implant systems have been developed. These can be distraction-based, compression-based, or growth-guidance and the details of these are discussed later in this technique.
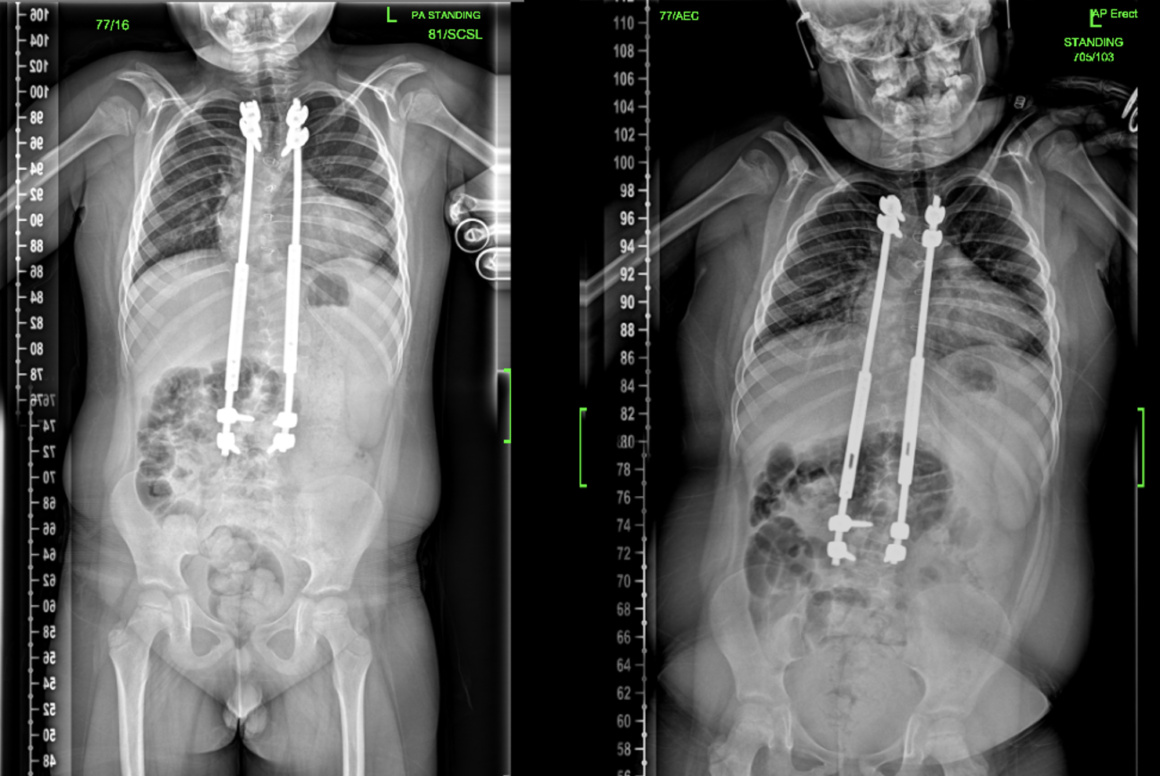
The patient involved here has distraction-based growing rods inserted; examples of this type of method include traditional growing rods and magnetically-controlled growing rods. Screws (or hooks) are inserted at the cranial and caudal extent of the deformity and rods then inserted between them. As the rods are inserted, a partial correction of the scoliosis is achieved but the patient does need to return to the operating theatre every six months for routine lengthening of the rods as they continue to grow. Since the rods are spanning a mobile section of the spine, there is a much higher complication rate using growing rods than following a fusion procedure; this could include rod breakage, screw or hook loosening, or junctional kyphosis and other deformity. Since the complication rate will increase with duration of time the implants have been in situ, it is important to attempt to avoid surgery until they are as old as possible and ensure all non-operative measures have been used. By delaying surgery for a year, this reduces risk of failure by 13% (Bess S, 2010). Complications rates of up to 58% have been described in spinal growing rods series.
Most children who have spinal growing rods inserted will be aiming to have them in place for at least two years. They need to have gained sufficient thoracic height by the time they are converted to a definitive spinal fusion so most will need to be at least 9 years old to ensure they do not develop thoracic insufficiency syndrome. If they still need further growth when the initial growing rods have lengthened as much as they can, then these are replaced with new growing rods to achieve more lengthening prior to a definitive fusion. The original growing rods systems are most commonly 4.5mm or 4.75mm rods; the definitive fusion will normally involve a 5.5mm system so the original screws will need to be revised as well at the time of revision surgery. At the time of revision surgery, the spine is often found to be a lot stiffer than a spine which has not been immobilised using growing rods; there may also be a pseudofusion across some of the spine due to previous exposure or contact with the implant. A surgeon, therefore, needs to be cautious when performing the definitive scoliosis correction in order to prevent screws pulling out due to the forces applied to them.
This case involves a patient who has DiGeorge syndrome (chromosome 22q11 deletion) and underwent surgery for Tetralogy of Fallot repair as an infant. He developed scoliosis when he was two years old and underwent plaster jacket therapy followed by using a removable brace. He was unable to comply with brace therapy due to learning difficulties and body habitus. His scoliosis, therefore, progressed and became severe. He had traditional spinal growing rods inserted six months previously when he was seven years old, and this technique describes his first routine lengthening.
The implant system featured uses pedicle screws cranially and caudally with a short and long rod in between them, which are connected together using the Medtronic Growth connector. The long rod is then gradually distracted out of the connector (this is described later in the technique). This system allows good contouring of the rod and is very cost-effective when compared to other implant systems on the market.
OrthOracle readers will find the following associated instructional techniques also of interest:
Anterior release of scoliosis (access by thoracotomy)
EDF(Elongation-Derotation-Flexion)/Mehta casting for Early Onset Scoliosis
Navigated posterior scoliosis correction for adolescent idiopathic scoliosis using Medtronic Solera system
Posterior Instrumented Adolescent Idiopathic Scoliosis Correction and Fusion (T4 to L4) using Globus CREO system
Scoliosis correction(neuromuscular): Anterior release and apical corpectomy
Scoliosis: Insertion of spinal traditional growing rods( Globus Marvel growing rod system) for early onset scoliosis
Skull-Skeletal Traction for correction of Adolescent Idiopathic Scoliosis (INTEGRA MAYFIELD infinity XR2 System)
T11 to L3 anterior scoliosis correction and fusion with the Globus Anterior Staple System
Author: Mr Stephen Morris FRCS (Tr & Orth).
Institution: Avon Orthopaedic Centre, Southmead Hospital, Bristol
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.eu

 00:00
00:00













